
By Tina S. Mehnpaine
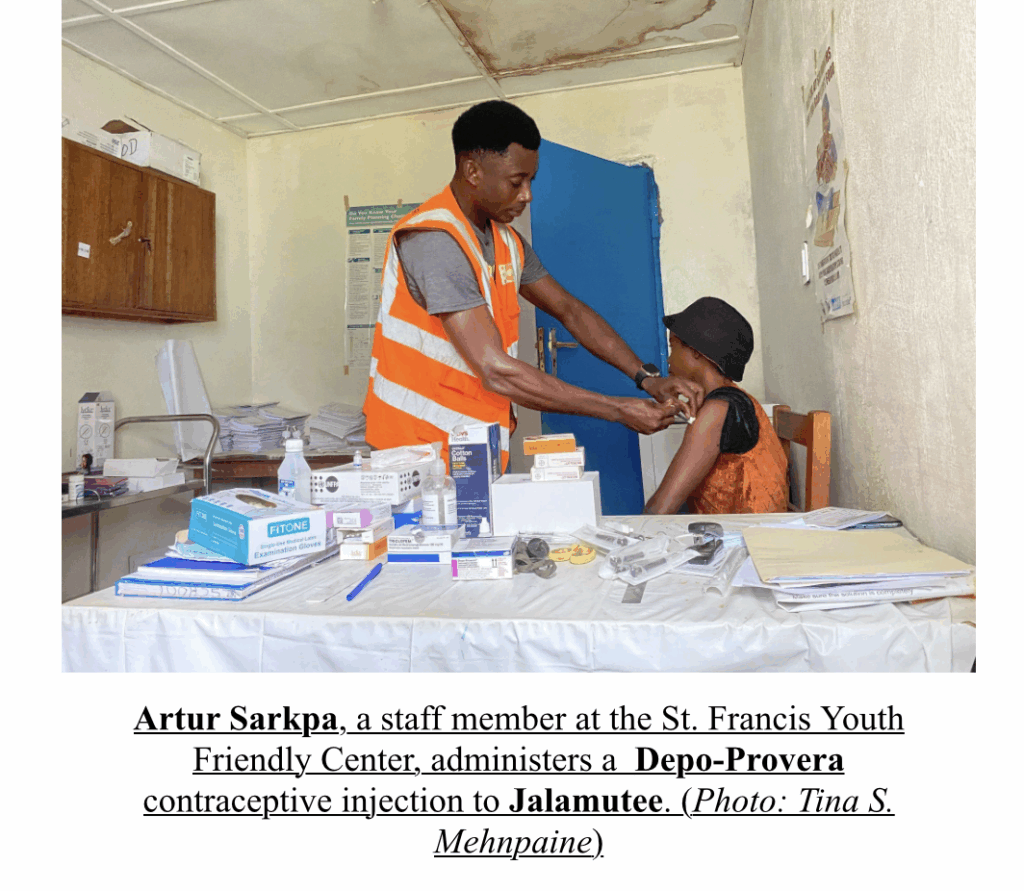
On a bright Tuesday morning in Cesto, Rivercess County, Angelina Jalamutee, 25, walks to the St. Francis Hospital Youth Friendly Center (YFC). She is there for her scheduled Depo-Provera shot, a family planning injection she receives every three months.
For Jalamutee, who had her first pregnancy at age 17, followed by a second at age 20, and dropped out of school after having two children, this medication is her sole protector against another unwanted pregnancy.
“I want to prevent myself from not getting pregnant because I already left behind in school,” she said. Her eyes are now set on completing high school by 2026, a critical first step toward her dream career as a medical doctor. As a future physician, she plans to ensure that sexual education becomes a standard part of the curriculum, making family planning information accessible to all children.
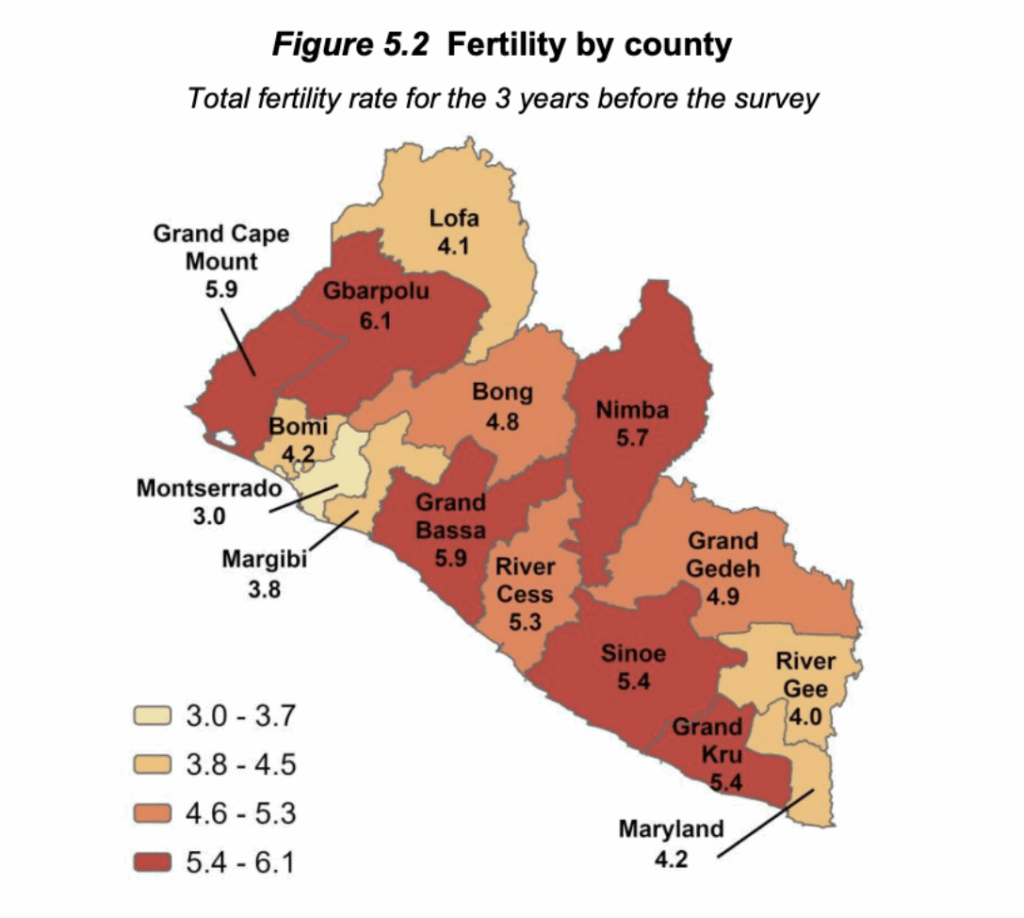
Jalamutee’s personal struggle with early pregnancy and its effect on her education are far from unique; her story reflects a national crisis. Teen pregnancies have been high since the end of Liberia’s civil conflict in 2003. The 2019-20 Liberia Demographics and Health Survey (LDHS) confirms the countyhas a high fertility rate, especially with women with no education.
Although the survey grouped women as aged 15 to 45, making it harder to focus directly on teenage girls, it still paints a worrying picture for those aged 15 to 19. Fewer than 1 in 100 girls in this age group have gone beyond high school. About 2 in 5 can read only part of a sentence, and nearly 3 in 10 cannot read at all.
Even more concerning, about 7 in 10 teenage girls have no access to any form of mass media, no radio, television, or newspapers, where most reproductive health information is shared in Liberia. Without access to these channels, many girls grow up without the necessary information to make informed decisions about their health.
As a result, girls between 15 and 19 have, on average, about four children. In rural areas like Rivercess, limited economic opportunities push many girls into early marriage or motherhood, forcing them to drop out of school. The percentage of girls who have started childbearing rises sharply with age — from just 1 in 25 at age 15 to more than half by age 19.
From the Liberia Demographics Health Survey (LDHS): The average number of children per woman declines with increasing education. Women with no education have an average of 5.3 children, as compared with 2.0 children among women with a higher education
To address this, the United Nations Population Fund (UNFPA) and the Embassy of Sweden jointly provided a sum of US$5.3 to start YFCs in the southeastern counties—Grand Gedeh, Grand Kru, River Gee, and Maryland. As the first-ever initiative since the country became peaceful, YFCs were designed to accommodate adolescents, as the name states—Youth Friendly Centers, providing a friendly and non-judgmental atmosphere for young girls and boys.

After years of implementation, the YFCs extended to Sinoe and Rivercess Counties, where girls like Jalamutee can walk into the facility for their preferred family planning care.
Jalamutee and her peers are reached through three main access channels: local communities, schools, and health centers. Out-of-school teens are reached via outreach and referrals, while students receive age-appropriate education through school health clubs and Comprehensive Sexual Education (CSE). The purpose is to achieve UNFPA’s three core transformative goals: ending preventable maternal deaths, unmet need for family planning among women, youth, and adolescents, and end gender-based violence and harmful practices, including Female Genital Mutilation (FGM).
The YFC program is not solely focused on adolescents, as it also offers services to adult women. “Things are hard, and having plenty of children will only make life harder,” says Martha Tweah, a mother of four, who has just renewed her implant, a birth control placed under the skin in the upper arm, which lasts for 3-5 years.
Teen pregnancies and abortion rights
Unwanted and unintended pregnancy among women and girls causes some to resort to abortion, which can lead to long-term health complications or death. Many, like Jalamutee, who fear these risks, were forced to become a teen mother. Already, Liberia’s tight restriction on abortion, which only allows it in cases of incest, fetal abnormality, or risk to the mother’s health, otherwise punishable by up to five years in prison; YFCs offer a vital preventive service.
The country’s updated Public Health law, passed by the House of Representatives, has been dormant in the Senate for years.
Senator Dabah M. Varpilah, chairperson of the Senate Committee on Health, informed participants at the country’s second annual conference on Sexual and Reproductive Health Rights (SRHR) that the bill, which is in the Senate, will surface on the floor in a very short period of time.
Regardless of abortion law, teen pregnancies are one of the barriers to adolescents achieving their full potential. Advocates say it delays girls’ education, increases poverty, lowers their self-esteem, and pushes girls further backward in society. “Some don’t even go back to school after childbirth,” says Bendu Kamara, Project Manager, Community Health Initiative (CHI).
This issue is at the center of Kamara’s advocacy, working with adolescents in communities, educating them about their bodies and the importance of family planning.
Jalamutee is fortunate to be one of the many adolescents in Rivercess County who can now access free family planning services. Her peers in Grand Bassa, a neighbouring county, do not have YFCs; their source of family planning comes from private drugstores or pharmacies, or they receive the medication as donations from NGOs.
As Donor Funding Declines, Liberia’s Youth-Friendly Centers Stand at a Crossroads
Liberia is a donor-dependent state with fragile infrastructural systems still rebuilding from a 14-year civil conflict. The health, education, and forestry sectors are hugely funded by donors; the YFCs are no exception. They operate on donations from global supporters like the Swedish embassy, and now the Irish embassy in Liberia solely supports the YFC programme in Rivercess County.
Gerard Considine, Ambassador of Ireland to Liberia, said these programs are intended to address gender inequality and help young girls achieve their full potential. Ambassador Considine added that the programs are aligned with the Irish government’s goal of setting a “better world” for women and girls.
A 2019 evaluation report of the Swedish and UNFPA joint-funded program—” Empowered and Fulfilled,” (E&F)—recorded progress against its ambitious targets, though the actual reduction in teenage pregnancies was 8 percentage points overall, falling short of the 10 percentage point target for each county. Specifically, the reduction was 20 percentage points in Grand Gedeh and 17 percentage points in River Gee, but only 2 percentage points in Grand Kru and Maryland.
This initial program was later extended to Rivercess and Sinoe Counties.
As lead implementer, UNFPA partners with local NGO such as Partners In Health (PIH) and the Young Men’s Christian Association (YMCA) to coordinate the YFCs’ activities among staff. These local organizations, including the YMCA, oversee stipend disbursement and staff management.
UNFPA, like most UN agencies, is firm on achieving its goals globally. Initiatives like the YFCs are a key strategy for young girls overcoming high contraceptive costs and helping them to make informed choices about their sexual and reproductive health. Similar YFC programmes exist in Asia, Pakistan, Tanzania, Syria, Nigeria, and Malawi.
“Teen pregnancies have reduced here,” said Doris Gizzie, Rivercess County’s Reproductive Health Supervisor.” Although a survey was last conducted in 2019-20, Gizzie believes many girls fully understand their sexual health and options for preventing pregnancies since the adoption of YFCs in Liberia.
However, despite these interventions, fertility is still high. Currently at 4.2 per woman, one in three births remains mistimed or unwanted, and adolescent fertility in the country remains one of the highest in West Africa at 30%.
Leonard Kamugisha, UNFPA Liberia deputy Country Representative, said the stats are still high because programs like the YFCs are not available in all parts of the country. He recommends YFCs as a national program that is “domestically funded” by the Liberian government in all fifteen counties. “International funding is declining,” he said.
Liberia suffered a big blow this year when one of the world’s major funders, the USAID, shut down operations, affecting several projects and programmes. Already, USAID-funded Youth Friendly Corners in Uganda have shut down, leaving the fight against teen pregnancies uncertain.
Kamugisha believed this should be a wake-up call to the Liberian government to take ownership of the program. Many of the staff assigned to the YFCs are volunteers. Tapitta M. Walker, a service provider at Fern River district clinic, said she has been volunteering for two years, but hasn’t been enrolled on the government payroll.
Leemu Nuch Walker, the Ministry of Health (MOH) Reproductive Health Coordinator, said volunteers are now being enrolled on the government payroll, although not all of them.
A Mother’s Joy
For parents like Mama Tugbeh from Kru Town, YFCs are a source of relief and pride. She says that with the YFCs present, teen girls are no longer succumbing to early motherhood.
Tubeh is a direct beneficiary. Early this year, her own 15-year-old daughter came to her asking to start family planning. “I held her hands and took her there myself,” she said.
“Since she started, there have been no problems,” Tugbeh added. Her daughter, who is in eighth grade, also dreams of becoming a medical doctor. “I am so proud of her. If this youth-friendly center wasn’t here, she might have become pregnant, and it would have become my burden.”
She encourages other parents to embrace family planning, pushing back against the myth that family planning damages young girls’ hormones or causes complications when they become women and are ready to have children. Many parents are skeptical about allowing their children to take family planning medication because of these myths, and can be abusive towards girls who choose these precautionary measures.
Yet discrimination and bullying force many women and girls to secretly use family planning methods from local drugstores or pharmacies without a proper prescription or education on the side effects, therefore putting themselves at risk. So when the medication fails, they discourage others from family planning.
Tugbeh also pushed back against the misconception that providing family planning education for young girls encourages early sexual activities.
But Martha James, a mother of five, believes that fear can be a natural preventive. According to her, family planning promotes engagement in sexual activities in young people because it removes the fear of unwanted pregnancies. James faced complications during her last child’s delivery, which she blames on the contraceptives she was taking at the time. “I face a problem with the sore,” James says.
From this experience, she vowed not to take family planning again. Now, her eighteen-year-old daughter, Fatu, has decided not to take family planning either. “I am not stopping her from taking family planning, ” says James. “She’s 18, and can make her own choice.”
From Beneficiaries to Advocates
Jalamutee had no plan to become a teenage mother. At age 16, she found herself in a circle of female friends who already had boyfriends. So when a boy asked to be her boyfriend, she gladly accepted, and within a year, she became pregnant with their first child. Three years later, she became pregnant with her second child.
“I stopped going to school because I had no one to help me take care of my children,” the mother of two recalled.
It was after her second child that she began taking family planning, initially the Implant, which she changed to the Depo Provera due to bleeding. She’s now on the front line, encouraging her peers and young ones to choose family planning.
“Every time I find myself in a gathering with my friends, I talk to them about family planning,’ Jalamutee says, who says she sometimes gets verbal attacks from those opposed to it. “But I don’t get angry. I will continue to speak and encourage young girls,” she vowed.
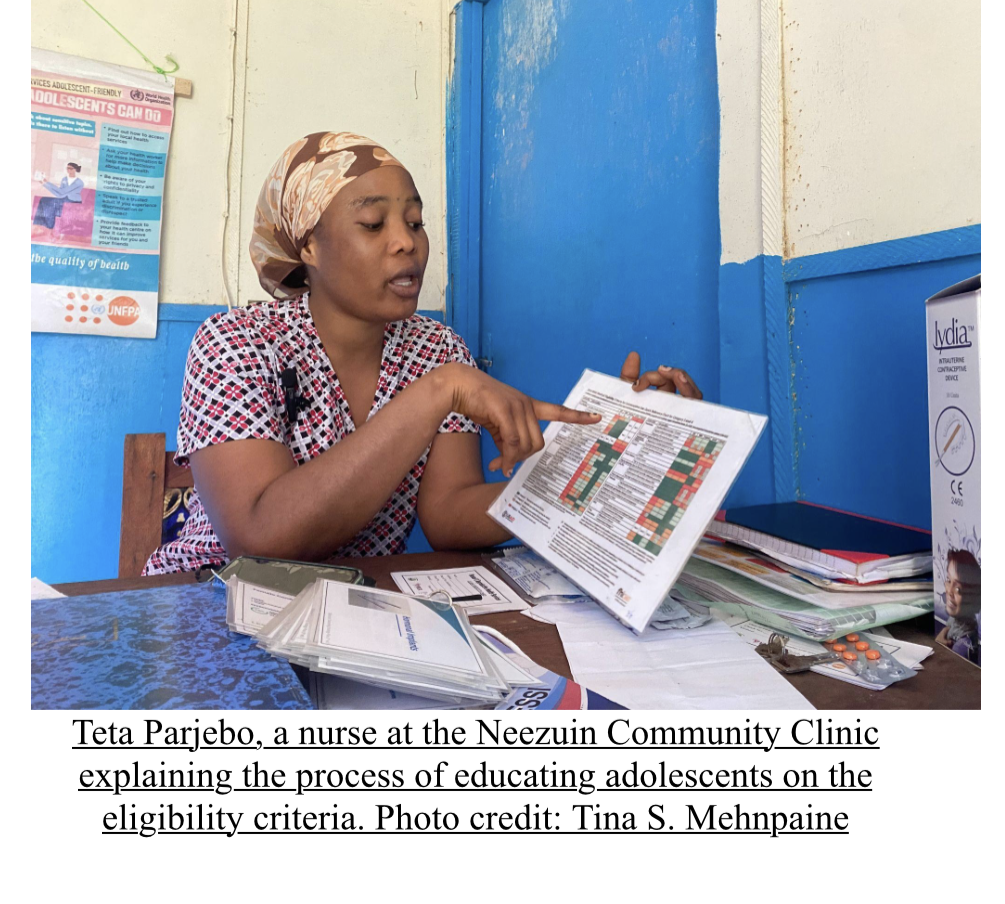
Princess Tamba 17, who lives in the Neezuin district of Rivercess County, is a beneficiary of the YFC initiative operating at the community clinic. Tamba, who is already a mother of one and a tenth-grade student, now uses her personal experience as a powerful lesson and clear example for her peers.
Using the same preventive medication as Jalamutee, she actively engages her community to discuss the benefits of family planning. She organizes and speaks to diverse groups, including adolescents, elderly women, and men, promoting awareness and informed choices.
“I tell them, if you get pregnant, the boy who pregnant you, will still be in school, while you’ll be the one staying home to take care of the baby,” she said.
Arthur Sarkpa, the 35-year-old nurse and staff member at the St. Francis Youth Friendly Center, resumes work at 8:00 AM every day. He attends to his patients, checking their cards to see if they are on schedule and if they have experienced any complications before moving forward with the injection.
“When they arrive, we make them feel welcome and comfortable. We show them all the options, explain the benefits and potential side effects, and let them choose what’s best for them.”
As part of his task, Sarkpa conducts outreaches in communities and works with the peer educators, mostly adolescents, to ensure clients don’t miss their return schedule day.
Low Pay, Stockouts, and Strained Systems Create Challenges for YFCs
Medications or “commodities,” as they are called, are supplied in the eighteen YFCs by the Ministry of Health and UNFPA. Staff assigned to these centers are recruited and paid from funds provided by the program. They are compensated for outreach efforts.
Sarkpa says the YMCA has stopped providing his monthly stipend of $100. Currently, he receives $45 every three months. This challenge was also voiced by Tapita Walker at the Fern River district. This has created a challenge, as staff are expected to work from 8 a.m. to 5 p.m. without proper compensation. Additionally, while the county provides supplies, there can be shortages of some methods, like implants.
Satta T. Massalay, the Liberian Ministry of Health School Health Coordinator, said YFCs experienced a stockout due to a flaw in the reporting system. “Staff will underreport the number of commodities they’ve used,” she says. “For example, if I give you 100 items to be used over three months, and you report that you’ve only used 50, the system will show you still have stock, even if you’ve used it all.” This underreporting causes delays in resupply.
Massaley, who works directly in the family Health Division, said there is a failure on the part of the health facility staff to request supplies promptly. They often wait until the stock is completely gone before placing an order, causing a gap in services at the clinics.
In an email, Emmanuel King, YMCA Communication Consultant, said the reduction in staff stipend was due to a drop in programme budget sanctioned by UNFPA, which was communicated to all staff at the onset of the year, through their working group forum and through the Rivercess county health team during their general inception meeting.
He added that the projected amount is paid every quarter. “I believe it is based on the number of services that are responding in such a manner. Meaning they divided the 91.7 to cover two service providers at each health facility and youth-friendly centers.”
Edited by Nelly Kalu
This story has been supported by the Solutions Journalism Network, a nonprofit organization dedicated to rigorous and compelling reporting about responses to social problems, http://solutionsjournalism.org
Editor’s note: This story is part of our effort to bring a Solutions Lens to investigative reporting on gender bias, particularly in reproductive health. Guided by four pillars—the response to the problem, the evidence for that response, its limitations, and the insights that can be replicated—we aim to show not just the problems, but how people are responding and building resilience in the face of challenges.

